
The 2001 WHO World Health Report highlighted the critical role that mental health (MH) plays in promoting the well-being of individuals, societies and nations at large. Globally, one in every three individuals experiences a mental illness during their lifetime, disrupting their MH. Approximately 970 million people had a mental health disorder (MHD) in 2017, accounting for 14.4% of years lived with disability (YLDs) from all causes. The actual MH burden is arguably far higher; when considering the overlap between psychiatric and neurological disorders, MHDs would account for 32.4% of total YLDs. Depression, anxiety, bipolar disorder, schizophrenia and other psychoses, dementia, substance use disorders, attention deficit hyperactivity disorder and developmental disorders, including autism, are the leading contributors to MHDs.
While MHDs affect people across all groups in society, the poor remain disproportionately impacted. This is particularly concerning in the 153 low- and middle-income countries (LMICs), where 85% of the world’s population resides and over 80% of MHDs occur.
The Mental Health Burden
Poverty, low socio-economic status, unemployment, low education levels, rapid urbanisation, internal migration, lifestyle changes, younger population demographics and discriminatory practices towards certain population subgroups all contribute to the high MH burden in many LMICs. Chronic conditions such as cardiovascular diseases, diabetes, cancer and respiratory diseases – collectively termed non-communicable diseases (NCDs) – often coexist with MHDs due to shared risk factors.
In LMICs, over 75% of people who require mental healthcare do not receive any form of intervention, compared with a “treatment gap” of only 35%–50% in high-income countries.
One of the Multiple Barriers to MH Care: Stigma
In mental health, stigma is sometimes more distressing and debilitating than the illness itself.
Stigmatisation manifests at the individual (intrapersonal), societal (interpersonal) and structural levels. For example, at the structural level, psychiatric professionals may simultaneously act as stigmatisers, recipients of stigma and agents of destigmatisation. In some countries, people with MHDs are less likely to be screened for comorbidities or receive medical visits due to factors such as limited knowledge of comorbidities among psychiatrists, attitudes among medical doctors and poor organisation of health services. Conversely, the presence of comorbid MHDs may be overlooked by physicians when significant physical disease is present. Knowledge gaps in the assessment and management of MHDs have been observed among non-psychiatric healthcare professionals and medical students in Latin America, Pakistan and Saudi Arabia.
Focus on the MH Context in Nepal
Despite the growing burden of MHDs in Nepal, a LMIC in South Asia, fewer than 10% of people with MHDs receive treatment. Structural barriers to care include the lack of mental health policies, low mental health budgets, shortages of trained human resources in primary healthcare settings and limited availability of medications. On the demand side, stigma related to mental disorders is widely reported as a dominant barrier to accessing care.
Conflicts between perceived causes and symptoms of mental disorders and culturally important values, combined with structural barriers, may lead to People With Lived Experience of mental disorders (PWLE) being labelled as violent, sinful or incapable of independent living. This may lead to human rights abuses such as chaining or confinement, discrimination in healthcare facilities, rejection in marriage proposals and exclusion from community or religious activities. Stigma related to MHDs appears to intensify when intersecting with gender, ethnicity and socioeconomic disadvantage. Women, widows, Dalits and people living in poverty are reported to face higher levels of stigma.
Another example concerns cultural and policy-related views of suicide. In Nepali culture, suicide is considered a sin and legally, it is treated as a criminal act. This shapes public perceptions of suicide attempt survivors as sinful or criminal. Such views contribute to internalised and public stigma, with individuals often seeing themselves as weak-minded or less suitable for marriage. This discourages treatment-seeking and treatment adherence.
Cultural Diversity and Implications for Mental Health
Stigma and discrimination vary across cultural and contextual settings. Cultural environments influence many aspects of mental disorders (see Table 1). Cultural factors such as perceived shame around a diagnosis of MHD, the desire to protect family reputation and personal dignity shape treatment-seeking behaviour. People with MHDs in LMICs such as India often present with somatic symptoms compared with the cognitive symptoms more commonly reported in Western countries. In LMICs where government support is minimal, a lack of family support due to stigma can lead to neglect of individuals with these conditions.
Traditional healers and faith-based communal practices are often preferred for addressing mental health crises in many LMICs, such as the Philippines. Filipino society places strong emphasis on hospitality and the family unit, which may delay help-seeking, with individuals enduring early symptoms until significant stressors arrive.
In Arab cultures, families and communities typically share responsibility for individuals with MHDs; however, stigma and the practical burden of care can, in some cases, lead to abandonment.
In Pakistan, children with developmental disorders report high levels of self-stigma stemming from cultural taboos surrounding MH and fear of rejection within joint family systems.
Egyptian patients with MHDs report higher levels of interpersonal stigma than self-stigma and express the need for support beyond psychiatric intervention.
Therapeutic models for addiction disorders in Mexico highlight the importance of gender, as stigma differs for women, men and people with diverse gender identities. Mexican women are nearly twice as likely to recognise MHDs and consider psychiatric interventions appropriate, whereas men often favour non-psychiatric approaches. Attributing MHDs to religious factors is also a recognised coping mechanism in Mexican culture.
Table 1. Key elements in the framework linking cultural factors and mental health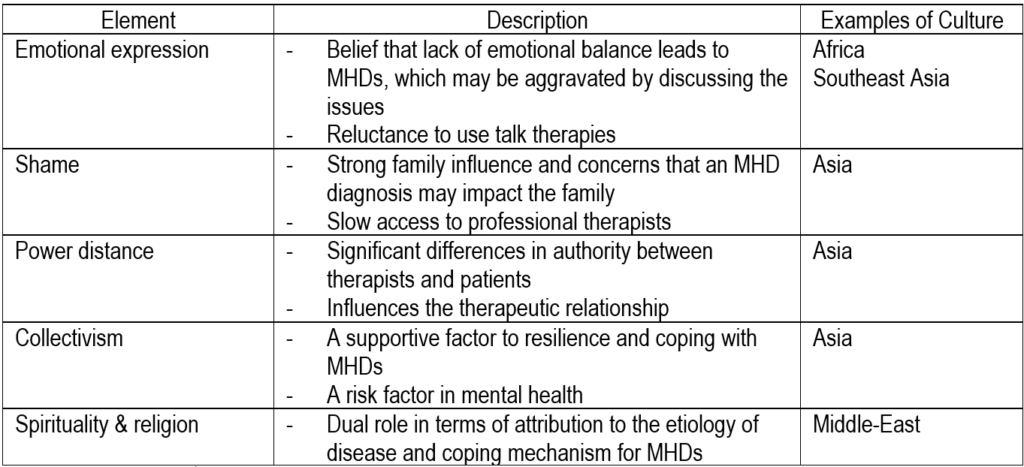 From Javed A et al. Reducing the stigma of mental health disorders with a focus on low- and middle-income countries. Asian Journal of Psychiatry 58 (2021)102601:1-8.
From Javed A et al. Reducing the stigma of mental health disorders with a focus on low- and middle-income countries. Asian Journal of Psychiatry 58 (2021)102601:1-8.
Conclusion
Mental health remains a culturally sensitive and neglected issue in LMICs. By 2030, depression is projected to become the third and second highest cause of disease burden in LMICs and middle-income countries, respectively.
Reducing cultural, social, financial, or gender-related barriers to service delivery is essential. This is reflected in increased implementation of family and community-based interventions to manage serious MHDs, employing destigmatising strategies such as therapeutic optimism, expanded support networks and stronger connections with formal and informal social services.
However, further research is needed to better understand the complexity of stigma processes and develop effective interventions targeting multiple domains. Future research should explore conceptual models that can inform study design, create culturally adaptive stigma assessment tools, and examine the forms and drivers of structural stigma. More intervention research is also needed to identify robust stigma-reduction strategies.
Veronique Ropion
Director Marketing & Communication, Pharmalys
Sources:
- Brooks C et al. Using evidence in mental health policy agenda-setting in low- and middle-income countries: a conceptual meta-framework from a scoping umbrella review. Health Policy and Planning, 38, 2023, 876–893.
- Gurung D et al (2022). Stigma against mental health disorders in Nepal conceptualised with a ‘what matters most’ framework: a scoping review. Epidemiology and Psychiatric Sciences 31, e11, 1–18. https:// doi.org/10.1017/S2045796021000809.
- Javed A et al. Reducing the stigma of mental health disorders with a focus on low- and middle-income countries. Asian Journal of Psychiatry 58 (2021)102601:1-8.
- Wondimagegn D, Pain C, Seifu N, et al. Reimagining global mental health in Africa. BMJ Glob Health 2023;8:e013232. doi:10.1136/ bmjgh-2023-013232.









